WPW - Ventricular Preexcitation Syndrome
Premature ventricular excitation is due to the ventricle is prematurely excited by the impulse more rapidly travel through the muscular connection(s) between atrium(atria) and ventricle(s) outside the specialized conducting tissue, the accessory pathway(s)
Different pathways. Atrioventricular (Kent); Atriohisian; Nodoventricular; Fasciculoventricular. [illustration - available soon]
Pathway location and localization. [illustration - available soon]. A patient can have more than one pathway.
Characteristic [Case1], [Case2-1], [Case3]. [Case4]Other findings:
- Short PR (<120 ms)
- Wide QRS. Early - Delta wave.
- Abnormal repolarization
- May produce pseudo infarction Q wave [Case2]; [other causes of pseudo Q wave]
- May create abnormal QRS voltage and direction Abnormal axis on frontal plane (LAD in case 2 and RAD in case 4), and abnormal QRS direction in precordial leads. (5) Predominant R wave in V1 (R/S ratio >1 in V1) in case 1 and case 4.
- Varying degree of preexcitation. [Case2], [Case3]
- Masking other causes of abnormal repolarization [Case1], [Case2-2], [Case3]. [Case 4]
Clinical significance
- A substrate for development of atrio-ventricular reentrant supraventricular tachycardia (macro-reentry)
Atrial fibrillation and atrial flutter with rapid antegrade conduction througth the accesory pathway is a serious condition. It may lead to ventricular fibrillation.
Supraventricular tachycardia
- AV reentrant (reciprocating) tachycardia [diagram - available soon]. vs AVN reentrant tachycardia [diagram - available soon]
- Othodromic (with or without bundle branch block). (ECG1), (ECG2), (ECG3),
- Antidromic (ECG1)
- P wave position and direction (compare AV reentrant to AVN reentrant tachycardia). No P; Short RP; Long RP; with LBBB
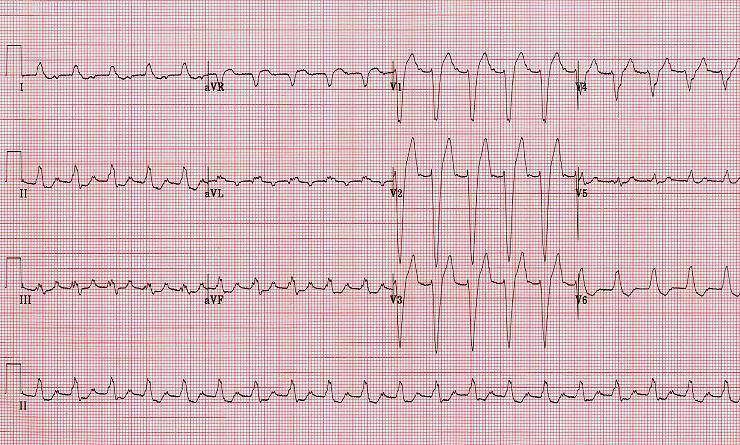
Atrial fibrillation with antegrade conduction through accesory pathway. [ECG1]
Atrial flutter with antegrade conduction through accessory pathway. [ECG1]
{kind=link}