 | |
| II  V1 V1 | |
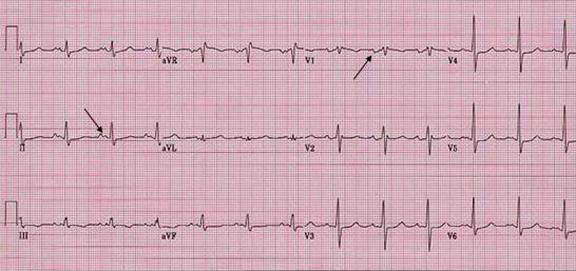
| LA abnormality. | |
| P mitrale is notched and wide P wave in lead II. The two peaks should be apart > 0.04 sec. P wave in V1 frequently has left atrial abnormality pattern as well. | |
| Patient. 51 year old female with the diagnosis of rheumatic mitral stenosis of moderate degree. Echocardiogram showed left atrial size of 6.5 cm, and mild pulmonary hypertension. She has recurrent atrial fibrillation. | |
| P wave abnormalities. There are wide range of variation of P wave abnormalities since several factors may effect the P wave. These include: Anatomic cardiac position to the anterior chest wall, state of autonomic influence, intra and/or interatrial conduction abnormality, atrial pressure and/or volume load, atrial diseases, electrode positioning (precordial lead). The diagnostic sensitivity are poor. | |
| LA abnormality, RA abnormality, or Intra/inter atrial conduction defect are better term than LA enlargement or RA enlargement. | |
|
LA
abnormality | RA
abnormality |
|
• Prolonged P wave >120 ms (0.12 sec). • Notched P wave in lead II ( P mitrale). The 2 peaks should be apart >0.04 sec. • Terminal negative P wave in lead V1 area >0.04 (amplitude in mV x duration in second). • Left shift of P wave axis on frontal plane (from +45 and +60 to -30 and +45) | • Peaked
P wave in lead II (inferior leads) > 2.5 mV. • Initial positive P wave in lead V1 amplitude >1.5 mV and area >0.06 (amplitude in mV x duration in second). • Right shift of P wave axis on frontal plane (from +0 to +75 to more than + 75) |