 |
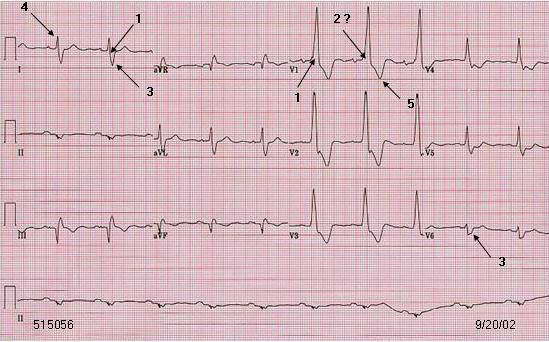
1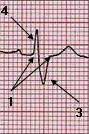 V1 V1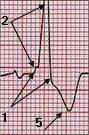 V2 V2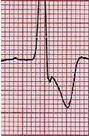 V6 V6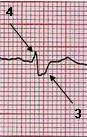 |
Comment:
Wide S wave in lead I and V6 is important. |
| RBBB. Less typical. |
| The r and s wave are very small and appears like a little shoulder in V1 and V2. Other abnormalities are inferior MI, indetermined axis on frontal plane. High R' may be due to coexisting right ventricular pressure and volume overload or posterior MI in this patient, although this ECG pattern may be found without the conditions mentioned. |
| Patient. 73 year old female S/P CABG twice, 1985 and 1996. She has had MI and coronary artery interventional treatment. Echocardiogram showed significan MR, moderate severe pulmonary hypertension and mild right heart enlargement. The LV size is normal with ejection fraction about 45%. |
|
Criteria for Typical
RBBB Other
abnormalities: |
| Go to RBBB menu. Go to QRS menu. Go to main menu |